
3.1 Recognition of Abuse and Neglect
This policy was last reviewed in July 2023 - changes to statutory guidance Working Together to safeguarding children may lead to further changes of this policy.
Date of next review: July 2025
Contents
- The Concept of Significant Harm(Jump to)
- Categories of Abuse and Neglect(Jump to)
- Risk Indicators(Jump to)
- Recognising Physical Abuse(Jump to)
- Recognising Emotional Abuse(Jump to)
- Recognising Child Sexual Abuse(Jump to)
- Recognising Neglect(Jump to)
The Concept of Significant Harm
| 3.1.1 | The Children Act 1989 provides the legal framework for defining the situations in which a local authority must make enquiries about what, if any, action to take to safeguard or promote a child's welfare. |
| 3.1.2 | Section 47 of the Act requires that if a local authority has 'reasonable cause to suspect that a child who lives or is found in their area is suffering or is likely to suffer Significant Harm, the authority shall make, or cause to be made, such enquiries as they consider necessary…' |
| 3.1.3 | In Section 31 Children Act 1989 as amended by the Adoption and Children Act 2002:
There are no absolute criteria on which to rely to determine what constitutes Significant Harm. It is often a compilation of significant events, both acute and longstanding, which impact on the child's physical and psychological development. Children's Services must consider all the circumstances when determining whether a referral about abuse and / or neglect to a child satisfies the criteria for a section 47 Enquiry - for further details, please see Section 47 Enquiries Procedure. |
Categories of Abuse and Neglect
| 3.1.4 | Abuse and neglect are forms of maltreatment of a child. Somebody may cause or neglect a child by inflicting harm or failing to act to prevent harm. Children may be abused in a family, or in an institutional or community setting, by those known to them or, more rarely by a stranger. They may be abused by an adult or adults or another child or children. |
| 3.1.5 | Working Together to Safeguard Children, 2018 includes definitions of the four broad categories of abuse that are used for recognition:
|
| 3.1.6 | These categories overlap, and an abused child does frequently suffer more than one type of abuse. This chapter provides definitions of these categories and information to help identify potential abuse and neglect and the required response. Professionals are encouraged to 'think the unthinkable' when working with families. Safeguarding requires professionals to think about the worst-case scenario (the unthinkable), even if it is then dismissed, based on evidence. |
Physical Abuse | |
| 3.1.7 | Physical abuse may involve hitting, shaking, throwing, poisoning, burning or scalding, drowning, suffocating, or otherwise causing physical harm to a child. |
| 3.1.8 | It may also be caused when a parent or carer fabricates the symptoms of, or deliberately induces illness in a child. This unusual and potentially dangerous form of abuse is described as fabricated or induced illness in a child (see Fabricated or induced illness (FII) and Perplexing Presentations (including FII by carers)). See also Recognising Physical Abuse |
Emotional Abuse | |
| 3.1.9 | Emotional abuse involves the persistent emotional maltreatment of a child, such as to cause severe and persistent adverse effects on the child's emotional development. |
| 3.1.10 | It may involve conveying to children that they are worthless or unloved, inadequate, or valued only insofar as they meet the needs of another person. It may include not giving the child opportunities to express their views, deliberately silencing them or 'making fun' of what they say or how they communicate. It may feature age or developmentally inappropriate expectations being imposed on children. |
| 3.1.11 | These may include interactions beyond the child's developmental capability, overprotection and limitation of exploration and learning, or preventing the child from participating in normal social interaction. It may involve seeing or hearing the ill-treatment of another. It may involve serious bullying, causing children to feel frightened or in danger or the exploitation or corruption of children. |
| 3.1.12 | Some level of Emotional Abuse is involved in all types of maltreatment of a child, though it may occur alone. |
Sexual Abuse | |
| 3.1.13 | Sexual abuse involves forcing or enticing a child or young person to participate in sexual activities, not necessarily involving a high level of violence, whether or not the child is aware of what is happening. The activities may involve physical contact, including penetration (for example, rape or oral sex) or non-penetrative acts such as masturbation, kissing, rubbing and touching outside of clothing. They may also include non-contact activities, such as involving children in looking at, or in the production of, sexual images, watching sexual activities, encouraging children to behave in sexually inappropriate ways, or grooming a child in preparation for abuse. Sexual abuse can take place online, and technology can be used to facilitate offline abuse. Sexual abuse may be part of criminal exploitation or gang activity. Practitioners must consider the increased risk of Honour Based Abuse (HBA) to victims of sexual abuse, particularly those of ethnic minority. Sexual Abuse is not solely perpetrated by adult males. Women can also commit acts of Sexual Abuse. |
| 3.1.14 | The Sexual Offences Act 2003 introduced a range of new sexual offences designed to address all inappropriate activity with children. |
| 3.1.15 | Child Sexual Abuse includes:
|
| 3.1.16 | In law, children under 16 years of age cannot consent to any sexual activity occurring, although in practice, young people may be involved in sexual contact to which, as individuals, they may have agreed. Children under 13 years cannot in law under any circumstances consent to sexual activity, and specific offences, including rape, exist for child victims under this age (see Sexually Active Children Procedure). |
Neglect | |
| 3.1.17 | Neglect is the persistent failure to meet a child's basic physical and/or psychological needs, likely to result in the serious impairment of the child's health and development. |
| 3.1.18 | Neglect may occur during pregnancy as a result of maternal substance misuse. Once the child is born, neglect may involve a parent or carer:
|
| 3.1.19 | Severe neglect of young children is associated with major impairment of growth and intellectual development. Persistent neglect can lead to serious impairment of health and development, long-term difficulties with social functioning, relationships and educational progress. Neglect can also result, in extreme cases, in death. |
Risk Indicators
| 3.1.20 | The factors described in this section are frequently found in cases of child abuse. Their presence is not proof that abuse has occurred, but:
|
| 3.1.21 | In an abusive relationship, the child may:
The parent or carer may:
|
| 3.1.22 | Consideration must be given to the impact on the care of the child of any issues/problems affecting parenting, e.g. domestic abuse, which may include physical violence; coercive and controlling behaviour, substance misuse, mental health problems, learning disabilities, childhood experiences of severe neglect or abuse; including sexual abuse. Consideration should be given to whether the parent can understand and predict risk and subsequently make appropriate decisions to protect their child from harm |
| 3.1.23 | The Home Office definition of Domestic violence and abuse was updated in May 2018 as: Any incident or pattern of incidents of controlling, coercive, threatening behaviour, violence or abuse between those aged 16 or over who are, or have been, intimate partners or family members regardless of gender (including gender identity) or sexuality. The abuse can encompass, but is not limited to:
|
| 3.1.24 | Controlling behaviour is a range of acts designed to make a person subordinate and/or dependent by isolating them from sources of support, exploiting their resources and capacities for personal gain, depriving them of the means needed for independence, resistance and escape and regulating their everyday behaviour. |
| 3.1.25 | Coercive behaviour is an act or a pattern of acts of assault, threats, humiliation and intimidation or other abuse used to harm, punish, or frighten their victim. |
| 3.1.26 | Staff should be aware of the potential risk to children of witnessing or being injured due to domestic abuse when a new partner is introduced into the family home or has substantial access to the children and is known as a perpetrator of domestic abuse. Individuals who have been in an abusive relationship are more likely to enter into other unhealthy or abusive relationship. If concerns are raised, an application under Clare's Law should be made as either a 'right to know' made by professionals or a 'right to ask', made by individuals, so the parent can understand any risks posed by their new partner to make an informed choice about the relationship. |
| 3.1.27 | Working Together to Safeguard Children, 2018, introduced the concept of Contextual Safeguarding which recognises that as well as threats to the welfare of children from within their families, children may be vulnerable to abuse or exploitation from outside their families. These extra-familial threats might arise at school and other educational establishments, from within peer groups, or more widely from within the wider community and/or online. These threats can take various forms, and children can be vulnerable to multiple threats, including exploitation by criminal gangs and organised crime groups such as county lines, trafficking, online abuse, sexual exploitation and the influences of extremism leading to radicalisation. |
| 3.1.28 | Staff should be aware of the potential risk to children when individuals, previously known or suspected to have abused children, move into or have substantial access in the household (see Risk Management of Known Offenders and Those who Pose a Risk). |
| 3.1.29 | It should be recognised that those who pose a risk to children often will not be honest with others. Staff should be mindful of this. Of particular note are carers who present a risk due to either fabricating or inducing illnesses within the children they are responsible for - see Fabricated or induced illness (FII) and Perplexing Presentations (including FII by carers) |
| 3.1.30 | Practitioners should, in particular, be alert to the potential need for early help for a child who:
|
| 3.1.31 | In schools, it is important that staff are aware that mental health problems can, in some cases, be an indicator that a child has suffered or is at risk of suffering abuse, neglect or exploitation. Only appropriately trained professionals should attempt to make a diagnosis of a mental health problem, however school staff are well placed to observe children day-to-day and identify those whose behaviour suggests that they may be experiencing a mental health problem or be at risk of developing one. Where children have suffered abuse and neglect, or other potentially traumatic adverse childhood experiences, this can have a lasting impact throughout childhood, adolescence and into adulthood. It is key that school staff are aware of how these children’s experiences can impact on their mental health, behaviour and education. |
Recognising Physical Abuse
| 3.1.32 | This section provides information about the sites and characteristics of physical injuries that may be observed in abused children. It is intended primarily to assist staff in recognition of bruises, burns and bites, which should be referred to Children’s Services and/or require a medical assessment |
| 3.1.33 | Further useful information can be found on the RCPCH website, about a series of systematic reviews defining the evidence base for the recognition and investigation of physical child abuse and neglect. The following are bruises/injuries/burns that should prompt a thorough assessment:
See 'Bruising' below for more information on bruising. Babies and young children can also sustain serious head and neck injuries as a result of abusive head trauma. Physical signs include reduced conscious levels, vomiting, irritability, apnoea (a pause/temporary stopping of breathing) or irregular breathing. The following are often regarded as indicators of concern:
For all young people, broader contextual safeguarding risks should be considered when there is an unexplained injury; consider individual vulnerabilities, e.g. exploitation into criminality/gangs/drugs/sexual; radicalisation; who has brought them/come with them for treatment. |
Bruising | |
| 3.1.34 | The Child Protection Evidence Systematic Review on Bruising (Royal College of Paediatrics and Child Health, 2020) found that bruising was the most common injury in children who have been abused. It is also a common injury in non-abused children, the exception to this being pre‑mobile infants where accidental bruising is rare (0-1.3%). The number of bruises a child sustains through normal activity increases as they get older and their level of independent mobility increases. Children can have accidental bruising, but the following must be considered as highly suspicious of a non-accidental injury unless there is an adequate explanation provided and experienced medical opinion sought:
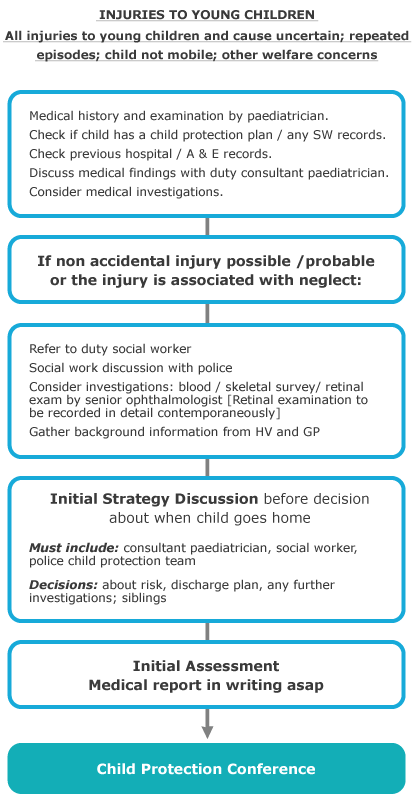
See also Bruises on children: Core info leaflet | NSPCC Learning see also Patterns of Bruising in Mobile Children See also Unexplained Injuries to Young Children |
Brief Resolved Unexplained Episode (BRUE), previously known as Acute Life-Threatening Event (ALTE) | |
| 3.1.35 | Most BRUEs have a medical or physiological basis, although a precise explanation is not always found. Some have unnatural causes, and assessment should always consider these through careful and detailed history taking, examination and investigations. Abusive Head Trauma (AHT) can present with irregular breathing, seizures or apnoeas. AHT must be considered in children presenting with BRUEs, and Child protection checks must be initiated for the child and any siblings. Any suspicions must be reported immediately to the duty social worker. |
| 3.1.36 | It is not possible to age bruises. |
Bite Marks | |
| 3.1.37 |
|
| 3.1.38 | A medical opinion from a forensic dentist/odontologist should be sought where there is any doubt over the bite's origin. |
Burns and Scalds | |
| 3.1.39 | It can be challenging to distinguish between accidental and non-accidental burns and scalds and will always require experienced medical opinion. Any burn with a clear outline may be suspicious, e.g:
|
| 3.1.40 | Scalds to the buttocks of a small child, particularly in the absence of burns to the feet, are indicative of dipping into a hot liquid or bath. |
Fractures | |
| 3.1.41 | Fractures may cause pain, swelling and discolouration over a bone or joint. |
| 3.1.42 | Non-mobile children rarely sustain fractures. |
| 3.1.43 | There are grounds for concern if:
|
Scars | |
| 3.1.44 | A large number of scars or scars of different sizes or ages, or on different parts of the body, may suggest abuse. |
Abusive Head Trauma (previously known as Shaken Baby Syndrome) | |
| 3.1.45 | Shaking and/or inflicting an impact injury on a baby often results in no visible external injury. Nevertheless, significant internal injuries may be caused, e.g. intracranial bleeding, brain injury, small fractures to the ends of the long bones, other fractures (such as ribs and neck) and retinal haemorrhages (a retinal haemorrhage is bleeding from the blood vessels in the retina at the back of the eye). Signs and symptoms can be non-specific, which may result in a delay in seeking advice. See also Unexplained Injuries to Young Children
|
| 3.1.46 | Young children and infants are highly vulnerable and may have a serious injury without obvious physical signs, e.g. shaking and/or impact injuries may result in internal head and other injuries. Nevertheless, significant internal injuries may be caused and result in:
|
| 3.1.47 | A full paediatric assessment must be carried out in suspected cases, including an ophthalmological examination, blood tests, and CT/MRI scans/skeletal survey (according to the RCR/RCPCH guidance). |
Self-Harming or injury caused by Siblings | |
| 3.1.48 | Caution must be used when interpreting an explanation by parents/carers that an injury or series of injuries was self-inflicted or caused by a sibling. This is especially important in young or disabled children not able to offer a reliable explanation themselves. |
| 3.1.49 | Due consideration must be given to the possibility that the injury may:
|
| 3.1.50 | In these circumstances, a referral to Children’s Services should be made following the Making a Referral Procedure |
{kind=link}
Recognising Emotional Abuse
| 3.1.51 | Emotional Abuse may be difficult to recognise, as the signs are usually behavioural rather than physical. |
| 3.1.52 | Emotional abuse is an extremely damaging form of abuse, which may occur in isolation or may co-exist with neglect and other forms of abuse. |
| 3.1.53 | Recognition of Emotional Abuse is usually based on observations over time and the following offer some associated indicators: Parent / Carer and Child Relationship Factors
Fabricated or induced illness falls under the wider umbrella term of emotional abuse. Cases of both FII and perplexing presentations also often involve or occur in association with other forms of abuse, particularly the various forms of emotional abuse. See also 8.21 Fabricated or induced illness (FII) and Perplexing Presentations (including FII by carers) | Sussex Child Protection and Safeguarding Procedures Manual Child Presentation Concerns
Parent / Carer Related Issues
Contextual factors may include:
|
Recognising Child Sexual Abuse
Please also see: | |
| 3.1.54 | child sexual abuse often remains hidden and is the most secretive and difficult type of abuse for children and young people to disclose. It may be particularly difficult to disclose abuse by a sibling. Many children and young people do not recognise themselves as victims of sexual abuse - a child may not understand what is happening and may not even understand that it is wrong. As a result, this type of abuse is considered to be under-reported. |
| 3.1.55 | Where there are any concerns about the sexual abuse of a child in a household, consideration must be given to the possibility that other children in the household may also be at risk. |
| 3.1.56 | Sexual abuse often occurs in conjunction with the other categories of child abuse, especially emotional abuse in order to maintain control and secrecy. It is also important to consider the possibility that children are being sexually abused in houses where neglect is happening. |
| 3.1.57 | Child sexual abuse can be perpetrated by any one of any gender and professionals are urged to use their professional curiosity. |
| 3.1.58 | There may be a range of signs of child sexual abuse but any one sign doesn't necessarily mean that a child is being sexually abused, however, the presence of a number of signs should indicate that professionals need to consider the potential for abuse and consult with others who know the child to see whether they also have concerns. Behavioural Indicators
|
| 3.1.59 | Physical Indicators
|
| 3.1.60 | The Centre of Expertise on Child Sexual Abuse uses a model proposed by Finkelhor and Browne, (1986) to describe four likely impacts of CSA:
In addition, the Centre highlights the impact that secrecy (including the fear and isolation this creates) and confusion (because the child is involved in behaviour that feels wrong but has been instigated by trusted adults) has on the child. In the long term, people who have been sexually abused are more likely to suffer with depression, anxiety, eating disorders and post-traumatic stress disorder (PTSD). They are also more likely to self-harm, become involved in criminal behaviour, misuse drugs and alcohol, and to commit suicide as young adults. |
Recognising Neglect
| 3.1.61 | Neglect of any type (physical, supervisory, medical, educational or emotional) remains the most common reason for a child to be the subject of a child protection plan in the UK Evidence of neglect is built up over a period of time and can cover different aspects of parenting. |
| 3.1.62 | Cases of both FII and perplexing presentations also often involve or occur in association with other forms of abuse, particularly neglect. |
| 3.1.63 | Child Related Indicators
|
| 3.1.64 | Indicators in the Care Provided
|
| 3.1.65 | Where there are any concerns about the neglect of a child in a household, consideration must be given to the possibility that other children in the household may also be at risk of neglect or abuse. |
| 3.1.66 | Neglect in teenagers aged 13-18: Read more : https://learning.nspcc.org.uk/media/1058/core-info-neglect-emotional-abuse-teenagers-13-18.pdf |
| 3.1.67 | Where there are any concerns about the neglect of a child in a household, consideration must be given to the possibility that other children in the household may also be at risk of neglect or abuse. |
| 3.1.68 | Obesity Obesity in children is an increasingly common problem in the general population and differentiating when there is a safeguarding issue can be difficult and complex. Neglect can result in poor supervision of food intake, or an inappropriate diet being offered to the child with resultant excessive weight gain. A sedentary lifestyle with limited opportunity for physical activity, when combined with an inappropriate diet, can result in excessive weight gain. It is important to take into account:
Excessive calorie intake is the cause of most childhood obesity. In a very small proportion of obese children, there is an underlying medical cause. The parent/carer is responsible for monitoring their child's diet and seeking appropriate advice/support if the child or adolescent is overweight or obese. The management of obesity in children, therefore, requires parental engagement to enable and support their child to adopt healthy eating patterns, participate in age-appropriate levels of physical activity and attend medical and dietetic appointments as necessary. Parental failure to engage with an appropriate management plan in a child who is severely obese and/or is developing serious complications of obesity should be considered a safeguarding issue. |