
15.1 Unexplained Injuries to Young Children
Last reviewed in July 2022
Date of next review - July 2025
Contents
Introduction
| 15.1.1 | |
| 15.1.2 | Physical injuries in young children may be life threatening and/or cause permanent neurological damage. Research and child safeguarding practice reviews (formally serious case reviews) highlight that children under 1 year old are especially vulnerable. Please refer to Evidence & reviews – RCPCH Child Protection Portal for key learning on a range of physical abuse injuries. |
| 15.1.3 | Any suspicious (unexplained) injury in a pre or non-mobile and/or pre or non-verbal child must be regarded with extreme concern including:
|
| 15.1.4 | Any injury and its explanation must be assessed in relation to the infant's/child's developmental abilities and the likelihood of the occurrence. The designation of the term “unexplained” should not influence staff into making assumptions that the injury is either accidental or non-accidental. All efforts must be made to establish an explanation for the injury which in turn may assist in determining whether or not the injury is accidental or non-accidental, and if a crime has been committed. |
| 15.1.5 | Young children and infants are highly vulnerable and may have a serious injury without obvious physical signs e.g. shaking and/or impact injuries may result in internal head and other injuries. Nevertheless significant internal injuries may be caused and result in:
|
Serious Unexplained Injury Strategy Discussion | |
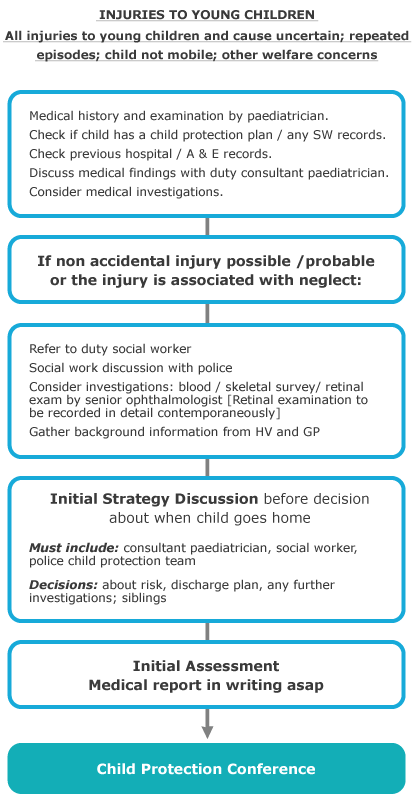
| 15.1.6 | If at the outset or before the conclusion of initial S47 Enquiries the mechanism for an injury to an infant or young child remains unknown, a serious unexplained injury strategy discussion should be convened. This Strategy Discussion should be undertaken as outlined in Strategy Discussion but must include additional considerations and the attendance of key staff.
|
| 15.1.7 | To review the current investigation and enquiries made to date;
|
| 15.1.8 | Participants Guidance as to who should attend strategy discussions is detailed in Strategy Discussions. In order for the serious unexplained injury Strategy Discussion to be effective the following personnel must be in attendance:
|
{kind=link}
Conclusion
| 15.1.9 | It may be necessary to hold more than one serious unexplained injury Strategy Discussion to finalise enquiries into an unexplained injury to an infant or young child. Where the S47 investigation is unable to determine how an injury was caused, the minutes of the final serious unexplained injury Strategy Discussion must record how each hypotheses/differential diagnosis was investigated and finalised or excluded. Participants to the final serious unexplained injury Strategy Discussion must all agree that all opportunities to determine the causation of an injury have been examined, and at the time of the serious unexplained injury Strategy Discussion there are no outstanding enquiries that can be undertaken. Such cases may require a fact finding. Should there be any professional disagreement during the course of the above procedure, reference must be made to the Resolution of Professional Disagreements |
Guidance
| 15.1.10 | |
| 15.1.11 | |
| 15.1.12 |